
.png)
Battle of the Filters: Immunoadsorption and Plasma Exchange Go Head-to-Head in Autoantibody Clearance - the CINEVAS TRIAL
- Dr. Medhavi Gautam
- Nov 3, 2024
- 8 min read
Written by: Dr. Medhavi Gautam
Imagine the body's smallest rivers—the delicate blood vessels—suddenly being engulfed by a wildfire, consuming them in silent destruction. This is the essence of small-vessel vasculitis, where necrotizing inflammation ignites these tiny vessels, often leaving no trace of the usual immune response by some traditional screening methods, a phenomenon known as pauci-immune. ANCA-associated vasculitis (AAV) is the name for these conditions, subcategorized as granulomatosis with polyangiitis (GPA), microscopic polyangiitis (MPA), and eosinophilic granulomatosis with polyangiitis (EGPA), all of which can lead to pauci-immune necrotizing crescentic glomerulonephritis, often involving the kidneys. Pauci-immune necrotizing crescentic glomerulonephritis (NCGN) notoriously results in a rapid decline in glomerular filtration rate (GFR). Serologic testing is essential for diagnosis; MPO- or PR3-ANCA positivity indicates ANCA-associated vasculitis (AAV). It’s important to note that ANCA negativity does not definitively rule out the diagnosis.

Figure 1: Adapted from : ANCA-associated vasculitis | Nature Reviews Disease Primers
The management of patients with ANCA-associated glomerulonephritis (AAGN) typically follows two key treatment phases. The first, known as the “induction” phase, focuses on reducing inflammation and reducing active disease to minimize renal injury. Once the disease is under control, treatment shifts to the “maintenance” phase, which primarily aims to prevent disease relapses. The approach to treating ANCA-associated Vasculitis (AAV) depends on the severity of the disease. AAGN is classified as "severe" AAV by definition, as it poses a threat to organs or life. Therefore, all patients with AAGN should receive treatment, regardless of the degree of renal injury. For example, in one study, 68% of 188 patients with a GFR of 20 mL/min or less experienced stabilization or improvement in renal function. Even among those with a GFR of 10 mL/min or less, 57% showed improvement. Additionally, patients requiring dialysis at or near presentation also had positive outcomes, with 55–90% being successfully weaned off dialysis here . However, for patients who remain dialysis-dependent after four months of induction therapy, the likelihood of recovering renal function drops to less than 5%. In such cases, immunosuppressive therapy should be discontinued unless there is extra-renal involvement that necessitates ongoing treatment.

The efficacy of plasma exchange (PEx) in ANCA-associated glomerulonephritis (AAGN) was first shown in the MEPEX trial (Figure 3), which found reduced rates of ESRD at 3 and 12 months but no difference in survival at 12 months or in long-term follow-up (median 3.95 years). The larger PEXIVAS trial (Figure 4) included 704 patients and found no significant difference in the primary composite outcome of death or ESRD between the PEx and non-PEx groups after 2.9 years.
A systematic review of 9 randomized controlled trials (RCTs) that enrolled 1060 patients with AAV found that though plasma exchange probably has little or no effect on mortality or disease relapse, it reduces the one-year risk of ESRD (along with the risk of infections as well!!). Based on the above evidence, the BMJ guideline panel agreed that patients at low risk of developing ESRD would consider the harms of PEx to outweigh the benefits, while high-risk patients would consider the benefits of PEx to outweigh the harms.

Figure 3: The MEPEX trial

Figure 4 : The PEXIVAS trial
Therefore, plasma exchange is only reserved for patients with severe renal impairment (SCr > 3.4 mg/dl), those requiring dialysis, or those experiencing diffuse alveolar hemorrhage with hypoxemia. Plasma exchange is also recommended for overlap syndromes involving ANCA-associated vasculitis and anti-GBM disease.
Plasma Exchange: Unveiling the Essentials
Plasma exchange (PEx) is an extracorporeal procedure in which plasma is separated from other blood constituents and subsequently removed from the patient by replacing with fresh frozen plasma or albumin solutions. Plasma exchange is a type of therapeutic apheresis, which is a medical procedure that separates blood components using centrifugation, filtration, or adsorption techniques. Within the realm of apheresis, immunoadsorption is a specialized form that specifically targets and removes antibodies and immune complexes (Figure 5,6).

Figure 5. Plasmapheresis schematic

Figure 6: Immunoadsorption schematic
The following table compares the salient features of these three procedures:

Immunoglobins associated with ANCA and their significance
Antineutrophilic cytoplasmic antibodies (ANCA) are primarily immunoglobulin G (IgG) antibodies identified using indirect immunofluorescence or enzyme-linked immunosorbent assays. Their removal can benefit patients due to their pathogenic role. IgG has a half-life of approximately 21 days, so merely halting its production with immunosuppressive agents would require weeks to lower serum levels. Therapeutic plasma exchange (PEx) effectively removes these antibodies quickly when used alongside standard immunosuppressive therapy.
Both centrifugal apheresis and membrane plasma separation are effective in IgG removal. PEx sessions are typically conducted one day apart to allow immunoglobulin redistribution, though daily sessions may be needed in emergencies like pulmonary hemorrhage. Besides removing antibodies, PEx can also eliminate inflammatory mediators, such as cytokines and complement components, and replenish plasma factors like factor H through fresh frozen plasma infusion.
The CINEVAS Trial
This article reports the findings of the CINEVAS trial, a prospective, non-randomised, multi-centre trial conducted across 8 university hospitals in France between January 2019 and August 2021. The study investigated the comparative efficacy of two apheresis techniques—immunoadsorption (IA) and plasma exchange (PEx)—in terms of autoantibody removal kinetics in patients diagnosed with ANCA vasculitis or anti-GBM disease.

Inclusion criteria
Age >18 years
A confirmed diagnosis of vasculitis (new or relapsing) associated with ANCA (either anti-proteinase 3 [PR3] or antimyeloperoxidase [MPO]) or with anti-GBM antibodies
Received corticosteroids and either cyclophosphamide or rituximab
Had an indication for apheresis (according to the investigator).
Exclusion criteria
Pregnancy or breastfeeding
Vasculitis without positive ANCA or anti-GBM antibodies
Severe anemia (hemoglobin level < 70 g/l)
Changed apheresis technique before the third session.
Primary Objective
To compare the reduction rates of autoantibody titers between the commencement of the first and end of the seventh apheresis session.
Secondary Objectives
The mean reduction rate in autoantibody levels per treatment session.
The number of treatment sessions required to achieve undetectable autoantibody levels or achieve reductions of 50%, 75%, or 90%.
The effects of IA and PEx on the levels of overall immunoglobulins, specifically examining the removal rates of IgG, IgM, and IgA.
Patient tolerance to both IA and PEx, monitoring any adverse effects or technical difficulties.
The overall impact of each technique on patient well-being, taking into account factors such as patient survival, kidney function, and disease activity.
Methodology
This trial compares two apheresis techniques—immunoadsorption (IA) and plasma exchange (PEx)—used to treat patients of ANCA vasculitis and anti-GBM disease, with the same technique consistently applied to each patient based on the center’s preference.
Apheresis procedures:
IA used Globaffin columns without substitution solute, treating 100 ml/kg of plasma per session.
PEx treated 60 ml/kg of plasma per session, with substitution using albumin and possibly fresh frozen plasma for coagulation purposes.
Blood tests:Blood samples were taken before and after each session to measure:
Anti-PR3, anti-MPO, anti-GBM antibodies
Total IgG, IgM, and IgA levels
Platelet, hemoglobin, fibrinogen levels, serum creatinine, and C-reactive protein These parameters were measured at days 15, 30, 6 months, and 12 months.
Vasculitis assessment:Vasculitis activity was assessed with the Birmingham Vasculitis Activity Score (BVAS) at inclusion, day 30, 6 months, and 12 months. The Vasculitis Damage Index was evaluated at similar time points.
Statistical methods:
Baseline characteristics were compared using chi-square or Fisher's exact tests for qualitative data and Mann-Whitney U tests for quantitative data.
Endpoints, including reductions in autoantibody levels, were compared using clustered estimates and tests to account for within-patient correlations (for multiple autoantibodies).
Outcomes (e.g., BVAS scores and technical parameters) were described using medians and quartiles and compared between IA and PEx groups using Mann-Whitney U tests.
The reduction rates of IgG, IgM, and IgA levels were analyzed similarly, also comparing centrifugation versus filtration techniques.
Software:Statistical analyses were performed using R (version 4.2.2), and a P-value of <0.05 was considered statistically significant.
Results
A total of 40 patients were initially enrolled in the study, but two were subsequently excluded—one due to negative autoantibody test results despite exhibiting symptoms typical of ANCA-associated vasculitis, and the other due to a change in treatment technique after the first two sessions. The final analysis included data from 38 patients, with 16 receiving IA and 22 receiving PEx. Table 1 shows baseline characteristics of patients.

Autoantibody Removal Kinetic
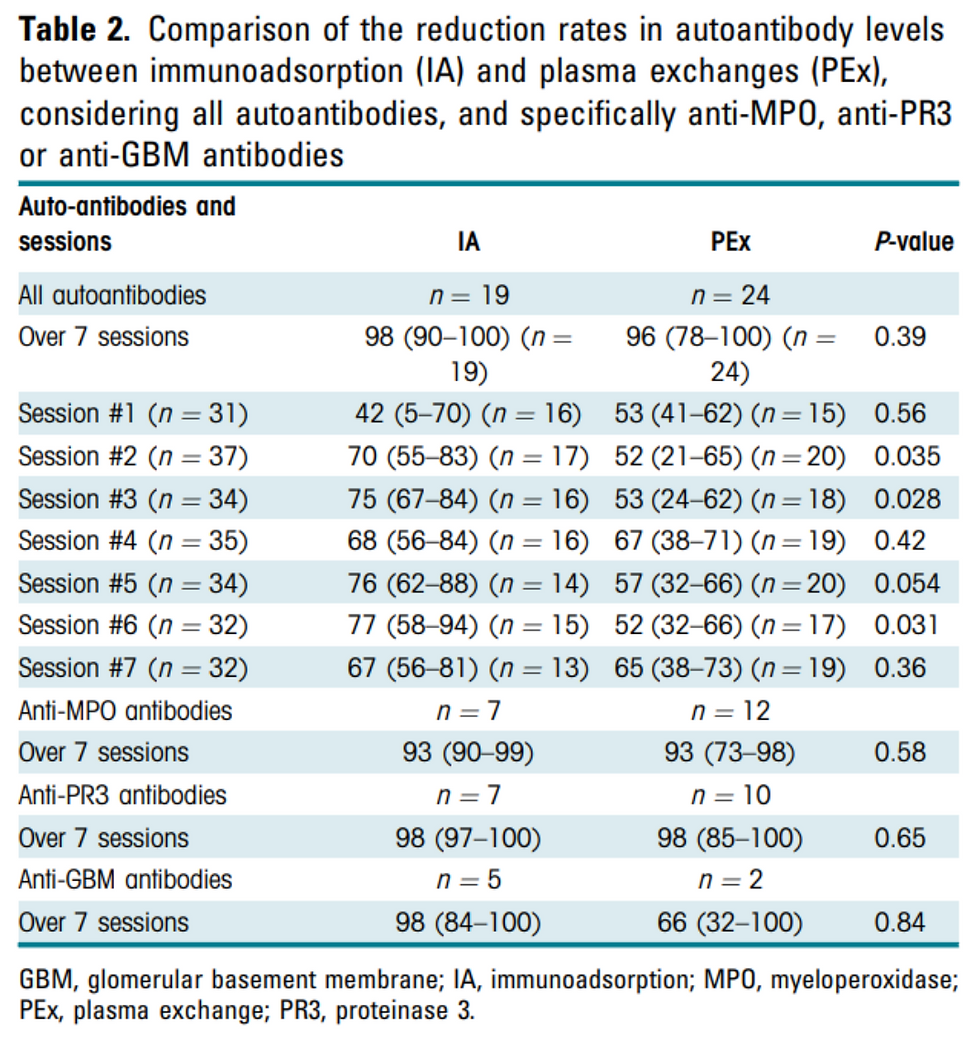
The kinetics of autoantibody removal, detailed in Table 2, showed no significant difference between immunoadsorption (IA) and plasma exchange (PEx) from the start of the first session to the end of the seventh session, whether analyzed by patient or antibody type. This was true for anti-PR3, anti-MPO, and anti-GBM antibodies.
Additionally, there was no difference between IA and PEx when comparing autoantibody reduction levels to baseline at the start of each apheresis session (Table 3).

Table 3: Comparison of reduction rates in auto-antibody levels at the beginning of each apheresis session, compared to the beginning of the first apheresis, between immunoadsorption (IA) and plasma exchanges (PEx).
The number of sessions required to achieve 50%, 75%, or 90% reductions, or undetectable levels of autoantibodies, did not differ between IA and PEx among patients who reached these goals within seven apheresis sessions (Table 4).

Table 4: Number of apheresis sessions needed to obtain 50%, 75% or 90% reductions or undetectable auto-antibodies, among patients who reached these objectives within 7 sessions.
Notably, regardless of whether IA or PEx was used, plasma separation by filtration resulted in a higher rate of antibody reduction compared to separation by centrifugation (Figure 1, Table 5).


Table 5: Comparison of reduction rates in total IgG, IgM, and IgA levels between plasma separation techniques (centrifugation or filtration) over 7 sessions. Results are presented as median [Q1-Q3].
Autoantibody reduction levels at 15 days, 30 days, 6 months, and 12 months are presented in Table 6.

Table 6:Comparison of the reduction rates in auto-antibody levels between immunoadsorption (IA) and plasma exchanges (PEx), considering all auto-antibodies, and specifically anti-MPO, anti-PR3 or anti-GBM antibodies, during the follow-up at 15 days, 30 days, 6 months and 12 months.
The reduction rate of total IgG was higher with immunoadsorption (IA) compared to plasma exchange (PEx), especially during the first four sessions. However, by the end of the seven sessions, IgG levels were similar between IA and PEx. Total IgM and IgA levels were significantly better preserved with IA throughout all seven sessions and remained higher in IA-treated patients after the seventh session compared to those treated with PEx. There was no difference in the reduction rates of total IgG, IgM, and IgA based on the plasma separation method, whether centrifugation or filtration.
Clinical outcome
There was no significant difference between immunoadsorption (IA) and plasma exchange (PEx) in the reduction rates of platelet counts (37% for IA vs. 36% for PEx) or fibrinogen levels (61% for IA vs. 76% for PEx) over seven apheresis sessions. Adverse events and technical issues are detailed in Table 4, showing that the plasma volume treated per IA session was almost double that of PEx, and IA required a larger volume of citrate. IA sessions were also longer.
There was no difference between IA and PEx in the evolution of the Birmingham Vasculitis Activity Index (BVAS) (Table 7).

Table 7 :Evolution of the Birmingham Vasculitis Activity Index (BVAS) over time, in patients treated with immunoadsorption (IA) or plasma exchanges (PEx).
3 IA-treated patients died (1 with anti-GBM and 2 with anti-MPO antibodies, all on dialysis at diagnosis) after 2.5, 3, and 4 months, respectively. No deaths occurred in the PEx group.
In the IA group, of the 8 patients requiring dialysis at the start, 3 died and 5 remained on dialysis. One additional patient required temporary dialysis on day 15 but later recovered kidney function.
In the PEx group, of the 5 patients needing dialysis at the start, 3 recovered kidney function, while 2 progressed to chronic kidney failure, with 1 on dialysis.
Among the 8 patients on dialysis at 12 months, autoantibody profiles included: 2 anti-GBM positive, 2 double positive for anti-GBM and anti-MPO, 1 double positive for anti-GBM and anti-PR3, 2 anti-MPO, and 1 anti-PR3 positive.
Conclusion :
This prospective non-randomized study found no significant difference in the reduction rates of ANCA or anti-GBM antibodies between immunoadsorption (IA) and plasma exchange (PEx) after seven sessions in patients with ANCA vasculitis or anti-GBM disease. Both techniques achieved over 90% reduction in autoantibodies. While IA showed a greater reduction in total IgG levels, the specific reduction in anti-MPO, anti-PR3, or anti-GBM antibody titers after one month was not significantly different between IA and PEx.
A key finding was that plasma separation by filtration led to greater removal of autoantibodies compared to centrifugation, despite similar removal rates for total IgG, IgM, and IgA. IA sessions treated larger volumes of plasma and lasted longer than PEx sessions, with a higher requirement for citrate but lower need for plasma infusion.
Patient outcomes were a secondary objective, but the IA group included more severe cases (e.g., patients requiring dialysis or with high serum creatinine levels). Among patients with anti-GBM disease, those in the IA group had worse renal prognoses. Despite these differences, there was no overall advantage of IA over PEx in terms of antibody reduction or clinical outcomes.



Comments