
.png)
Bleeding, Clotting, and Kidney Disease in Atrial Fibrillation: Can Factor XI Inhibitors Change the Game?
- Husam Alzayer MD
- Sep 5, 2025
- 8 min read
Updated: Sep 8, 2025
Reviewed by Sophia Ambruso, DO
Introduction
Bleeding and thrombosis represent one of the many paradoxes faced by patients with kidney disease. As kidney function declines, patients concurrently experience an increased risk of both bleeding and thrombosis. This creates a dilemma when attempting to start an anticoagulation strategy in patients with atrial fibrillation that is often challenging to resolve, even when considering individual patient risk, due to the absence of validated risk scores in this unique high-risk population. Factor XI is uniquely positioned because of its supportive role in thrombus growth and stabilization, without being essential for clot formation in response to tissue injury. This makes Factor XI inhibitors a promising option for preventing pathological thrombosis while avoiding an increased risk of bleeding. In this blog post, we will discuss how to assess the risk of thrombosis and bleeding in patients with advanced kidney disease, the current evidence regarding prophylactic anticoagulation in this population, and the promising role of Factor XI in this context.
The Hemostatic Paradox in Kidney Disease
With advanced kidney disease, there is an increased risk of thrombosis and bleeding. The risk of bleeding arises from platelet dysfunction and altered interactions between platelets and the vessel wall, due to the buildup of uremic toxins, as well as the systemic use of heparin during hemodialysis or the routine administration of anticoagulants or antiplatelet agents. The heightened risk of thrombosis stems from the chronic inflammatory milieu that patients with advanced kidney disease have, coupled with endothelial dysfunction that leads to ongoing activation of the coagulation cascade and platelet activation during hemodialysis. Against the backdrop of a higher prevalence of atrial fibrillation and its serious risk of developing ischemic strokes, initiating a prophylactic anticoagulation strategy can be challenging.
Atrial fibrillation, whether paroxysmal, persistent, or permanent, is a well-known risk factor for the development of embolic strokes. Physicians use the CHA₂DS₂-VASc and HAS-BLED scores to guide the assessment of the benefits and risks for patients when deciding on an anticoagulation strategy. However, the CHA₂DS₂-VASc score has not been validated in patients with advanced kidney disease. In fact, an observational study of nationwide Danish registries reported a 5.5-fold increased risk of stroke in patients receiving renal replacement therapy, even when the CHA₂DS₂-VASc was 0. Regarding the HAS-BLED score, it also did not perform well in predicting the bleeding risk for patients undergoing dialysis.
To provide further perspective, the risk of developing a venous thrombotic event in patients undergoing dialysis is 3 to 7 times greater than in those with normal kidney function. Moreover, their bleeding risk is approximately 100 times higher than that of the general population, a risk that escalates further with anticoagulant treatment. Additionally, while ischemic strokes are the most prevalent among those with chronic kidney disease, hemorrhagic strokes become increasingly common as kidney function declines and occur at a similar rate to ischemic strokes in the dialysis population.
This complex relationship between bleeding and thrombosis creates clinical and therapeutic uncertainty, set against a backdrop of insufficient data from clinical trials that have historically included a limited number of patients with an eGFR <30 ml/min/1.73 m2 and excluded those with end-stage kidney disease.
Ultimately, the decision to implement an anticoagulation strategy for patients with advanced kidney disease should be based on a thorough evaluation of benefits and risks, along with individual patient considerations. A more effective approach would be to utilize risk scores that have been developed and validated in the dialysis population to inform this decision. The Dialysis Risk Score focuses on factors significantly associated with stroke risk (previous stroke, diabetes, and older age) while ignoring factors that are not (hypertension and heart failure) in the Dialysis Outcomes and Practice Patterns Study (DOPPS). Another stroke risk prediction score is the Modified CHADS2 score, which outperformed five other scores, including the CHA₂DS₂-VASc score, demonstrating good and consistent performance across all kidney function strata. Notably, it also did not include hypertension and heart failure. Regarding bleeding risk, the BLEED-HD risk score, although not specifically developed with atrial fibrillation in mind, has been validated in the hemodialysis population and may provide a better insight into patients' true risk of bleeding.
Current Approaches to Anticoagulation in CKD
After deciding to use anticoagulation based on a patient-centered benefit-risk assessment, the challenge arises of selecting the appropriate anticoagulant. Currently, the choice is limited to direct oral anticoagulants or warfarin. Although only two options are available, the decision-making process remains complex. The use of direct oral anticoagulants has largely superseded warfarin in patients with non-valvular atrial fibrillation without advanced kidney disease, and has become the standard of care. However, this evidence may not be generalizable to patients on dialysis.
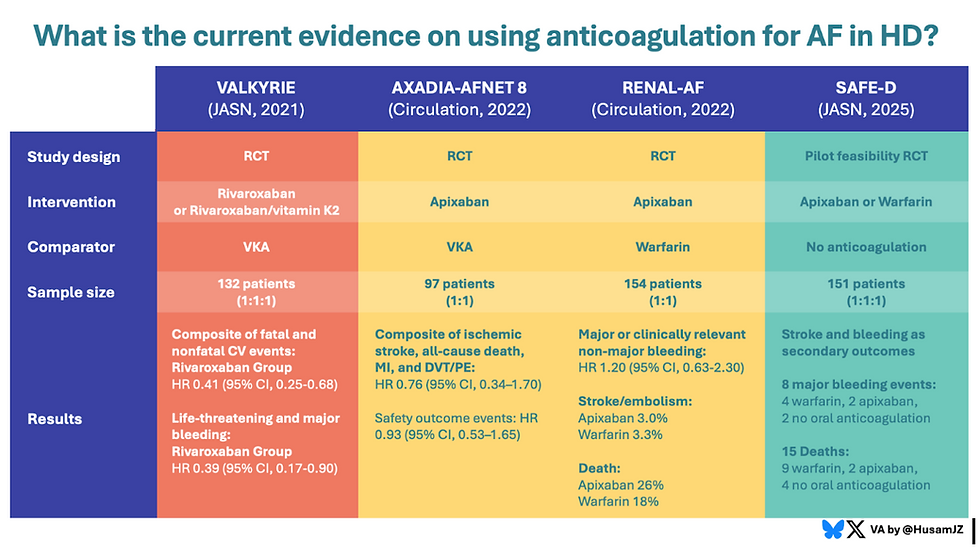
Apixaban and rivaroxaban are the only direct oral anticoagulants with data to support their use across the spectrum of kidney disease, up to dialysis. Rivaroxaban vs warfarin (VKA) was studied in a multicenter randomized controlled trial (RCT), the Valkyrie study in patients undergoing hemodialysis with atrial fibrillation. Although the study was considered an overall win for rivaroxaban, with significantly favorable results, it had a small sample size. Additionally, 25% of patients prematurely discontinued treatment and experienced suboptimal warfarin control, leading to fewer than 16% of patients maintaining therapeutic INR levels for at least 60% of the time.
Apixaban use, on the other hand, was evaluated in two prospective multicenter RCTs, published in Circulation, the RENAL AF and AXADIA-AFNET 8 studies. Both studies had limitations in terms of recruitment, which were not adequately powered to reach a conclusive result. However, a main objective was to assess apixiban's safety, which was similar across the two groups in both studies compared to VKA, despite patients receiving VKA being in the therapeutic INR range for less than 50% of the time.
This raises the question: if most patients on VKA in these trials were at sub-therapeutic levels, should we not also explore the possibility of not using an anticoagulation strategy at all in the absence of a safe intervention, especially in the setting of conflicting evidence?
This brings us to the SAFE-D trial (Strategies for the Management of Atrial Fibrillation in Patients Receiving Dialysis), which was a multicenter, parallel-group pilot randomized controlled trial (RCT) conducted at 28 centers in Canada and Australia. The primary objective of the trial was to demonstrate the feasibility of recruitment and protocol adherence, which it successfully achieved, and showed a reassuring safety signal, as major bleeding events and death were not higher in the no anti-coagulation strategy. The time in the therapeutic range for warfarin recipients was 58%, consistent with other studies. Further trials (NCT05679024 and NCT03862859) are currently recruiting to explore apixaban versus no anticoagulation.
Limitations of Warfarin in Dialysis
As demonstrated, warfarin is significantly more challenging to administer in patients undergoing dialysis than in those who are not. When not managed appropriately, the risk of bleeding can outweigh its benefits if the dosage is supratherapeutic. Additionally, the intended benefit of preventing thrombotic events diminishes when the dosage is subtherapeutic. A much-feared complication linked to warfarin use in dialysis patients is the development of calciphylaxis, a severe complication believed to result from warfarin’s inhibition of matrix Gla protein, a vitamin K-dependent protein that actively inhibits calcification; warfarin's use is also associated with major bleeding events, both of which are not uncommon. Furthermore, some studies do not show that the risk of stroke is lower when using warfarin in the context of atrial fibrillation in patients with ESKD; in fact, it appears to be higher.
Factor XI: A Novel Target in Coagulation
Factor XI plays an important role in the intrinsic clotting cascade, where its activated form (factor XIa) amplifies thrombin generation. It has been observed that patients affected by hereditary factor XI deficiency have a lower risk of developing venous thromboembolism and ischemic stroke; however, they rarely experience spontaneous bleeding, though phenotypic variability exists. These observations have spurred interest in targeting factor XI as a therapeutic strategy by uncoupling thrombosis prevention from normal homeostasis, enabling maximal anticoagulation without increasing the risk of bleeding.

Factor XI/XIa inhibitors are available in various forms, offering flexibility and convenience in dosing. These include:
Oral small-molecule inhibitors: Milvexian, Asundexian
Parenteral monoclonal antibodies: Abelacimab, Gruticibart (AB023), MK-2060 Osocimab
Parenteral antisense oligonucleotides (ASOs): Fesomersen, IONIS-FXIRx


Factor XI/XIa inhibitors have shown efficacy, safety, and non-inferiority to enoxaparin in preventing postoperative venous thromboembolism across several Phase 2 studies, including the FOXTROT, ANT-005 TKA, and AXIOMATIC-TKR studies. Additionally, the AXIOMATIC-SSP study demonstrated the safety of the factor XIa inhibitor milvexian, even when combined with clopidogrel 75 mg daily for 21 days and aspirin 100 mg daily for 90 days, for secondary stroke prevention in a Phase 2 trial, with a Phase 3 trial in development.
Phase 3 investigations have expanded into atrial fibrillation populations. The OCEANIC-AF trial compared asundexian to apixaban, but was halted prematurely due to a higher incidence of stroke and systemic embolism in the asundexian arm, despite fewer major bleeding events. Authors of OCEANIC-AF postulate the higher incidence of stroke and systemic embolism was related to it being an underdosed trial whereby a dose finding study was never performed prior, and that asundexian is a small molecule competitively inhibiting factor XIa only, positioning that near complete factor XI inhibition was not achieved. The AZALEA–TIMI 71 trial, published a few months later, compared abelacimab, a monoclonal antibody inhibiting Factor XI and Factor XIa, to rivaroxaban in patients with atrial fibrillation regarding major or clinically relevant non-major bleeding and was also stopped early, this time in favor of abelacimab, which resulted in a greater-than-anticipated reduction in bleeding events; the hazard ratio for 150-mg abelacimab vs. rivaroxaban was 0.38 [95% CI, 0.24 to 0.60], and for 90-mg abelacimab vs. rivaroxaban, it was 0.31 [95% CI, 0.19 to 0.51]; P<0.001 for both comparisons. Efficacy studies for abelacimab in atrial fibrillation are underway.
Overall, the safety signal for factor XI/XIa inhibitors in reducing bleeding is promising; however, further work is needed to determine which populations would benefit the most from these medications and for which conditions. For patients on hemodialysis, this was examined more closely in a systematic review of phase 2 trials published in KI Reports. Five studies involving 1270 participants received one of the following factor XI/XIa inhibitors, which were compared to a placebo:
Gruticibart: a monoclonal antibody that binds to the apple 2 domain of factor XI and blocks its activation by factor XIIa.
IONIS-FXIRx: an antisense oligonucleotide that blocks the hepatic synthesis of factor XI
Osocimab: a monoclonal antibody that binds the catalytic domain of factor XIa and inhibits its activity
Fesomersen: a ligand-conjugated factor XI-directed antisense oligonucleotide that blocks the hepatic synthesis of factor XI
The meta-analysis reported the following odds ratios for key outcomes (all vs. placebo):
Major and clinically relevant non-major bleeding: 0.80 (95% CI, 0.47–1.35)
Major bleeding: 0.51 (95% CI, 0.21–1.28)
Clinically relevant non-major bleeding: 0.90 (95% CI, 0.49–1.68)
Thromboembolic events: 0.66 (95% CI, 0.28–1.56)
All-cause mortality: 0.46 (95% CI, 0.15–1.40)
Although none of these outcomes reached statistical significance, the trends suggest a reduction in bleeding and thromboembolic risk, underscoring the potential value of further investigation in this high-risk population. Several ongoing studies involve factor XI inhibitors; however, the ones focused on atrial fibrillation and include patients with advanced kidney disease are LIBREXIA-AF, which compares milvexian, an orally active, specific small molecule inhibitor of factor XIa, to apixaban (NCT05757869), and LILAC-TIMI 76, which compares abelacimab to placebo in patients unsuitable for oral anticoagulation due to their high bleeding risk, but not yet on dialysis (NCT05712200). Additionally, another trial was recently completed and is awaiting publication on preventing AVG thrombosis and assessing the safety of MK-2060, an anti-Factor XI monoclonal antibody, in patients receiving hemodialysis (NCT05027074).
Conclusion
The use of anticoagulation mainly comes from the need to treat patients who develop thromboembolic events and to reduce the risk of ischemic strokes in those with atrial fibrillation. The adverse events associated with current anticoagulation strategies are not without risks, as advanced kidney disease is a risk factor for both bleeding and thrombosis, leading to therapeutic dilemmas with limited evidence to guide safe practices. Factor XI inhibitors offer a promising shift in hemostasis management with a safer bleeding profile. However, more data are needed to confirm their effectiveness, including real-world evidence on clinically significant outcomes.



Comments