
.png)
Towards new ways of assessing kidney function. Where to look to improve?
- Elba Medina MD
- Oct 24, 2025
- 8 min read
Written by Elba Medina
Reviewed by Brian Rifkin;Sophia Ambruso
Today, current methods for measuring kidney function, due to several critical limitations, need to be reimagined. In the reimagining Kidney Function Assessment Workshop, organized by the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), experts met to deliberate current limitations and potential advances in the quantification of kidney function. Read the executive summary and watch the meeting video for more information.
The kidneys’ functions are numerous and diverse, making it difficult to develop a biomarker to evaluate each function individually and comprehensively to establish a specific therapeutic target. We use estimated glomerular filtration rate (eGFR) and uACR (urinary albumin-creatinine ratio) as our main biomarkers. However, despite their widespread use, they lack specificity and fail to clarify some diagnostic difficulties. The examples below illustrate the shortcomings of contemporary kidney function assessments, whereby two people can have the same kidney function metrics with substantially different scenarios.

Figure 1. Infographic adapted from Toward a Comprehensive Framework for Kidney Function Assessment: A Comprehensive Approach from Reimagining Kidney Function Assessment Workshop
Beyond eGFR: Improving the accuracy of GFR measurement.
Glomerular filtration rate (GFR) is the best overall indicator of kidney function, although it is not comprehensive. Measured GFR (mGFR) is usually estimated using formulas that use endogenous biomarkers. Direct measurement, using measured urinary or plasma clearance of exogenous filtration markers, is preferred in specific clinical situations needing higher accuracy; however, despite being more accurate than eGFR, it is underused in clinical practice due to the need for standardization, difficulties associated with collection, lack of reimbursement, policy support, and limited availability of some filtration markers. Iohexol is the current marker of choice, non-radioactive, widely used, and readily available.
Key Research Question. How can standardizing iohexol plasma disappearance protocols improve the accuracy and reliability of measured GFR in clinical and research settings?
The Chronic Renal Insufficiency Cohorts (CRIC) study found that mGFR may not necessarily provide a better prediction of outcomes in CKD, despite the fact that mGFR has long been considered the “gold standard” measure of kidney function. However, there are differences between mGFR vs True GFR due to errors in clearance methods, imperfect marker properties, assay inaccuracies, and biological variability. In healthy individuals, circadian rhythms alone can produce up to 33% variations in GFR. There is a need to find an accurate, precise, reproducible, and reliable assessment of GFR. eGFR is affected by marker generation rates, tubular processing, extrarenal elimination, and assay errors. Serum creatinine and cystatin C measurements of eGFR can produce inconsistent results, which may be impacted by the non-GFR determinants unique to each marker. So it's necessary to look at new methods and/ or equations for the development of more reliable new tools and to reduce reliance on any single biomarker.

Table 1. Infographic adapted from Toward a Comprehensive Framework for Kidney Function Assessment: A Comprehensive Approach from Reimagining Kidney Function Assessment Workshop. Effects of non-GFR determinants on creatinine and cystatin C as endogenous filtration markers.
Key Research Question. How can eGFR assessment be improved by addressing variability and identifying biomarkers to better reflect true GFR across clinical scenarios?
Researchers are currently evaluating new proteins and low-molecular-weight metabolites (a panel of filtering markers) that can help reduce the impact of non-GFR determinants on any individual marker. Recently, a novel fluorescent GFR tracer agent, relmapirazin, was evaluated for its potential in transdermal detection of real-time GFR. This emerging technology holds promise for accurate, point-of-care renal function assessment, offering an
advantage over biomarkers such as serum creatinine, which are often delayed in reflecting acute changes in GFR. Real-time monitoring could support theranostic evaluations, particularly in acute care and early intervention scenarios.
The adoption of new technology also has the potential to reduce the misclassification of CKD stage, currently estimated to affect between 30%-50% of patients when standard equations, based on serum creatinine or cystatin C, are used.
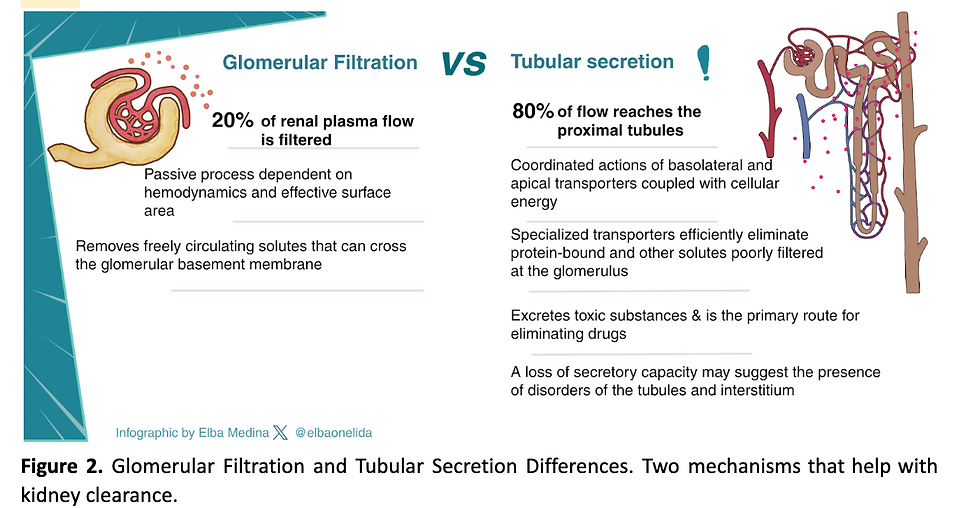
Kidney clearance
Two main mechanisms of kidney clearance occur in the kidney: glomerular filtration and tubular secretion, which have different physiologic mechanisms but are complementary. Tubular secretion is the primary route of elimination for protein-bound substances that the glomerular basement membrane cannot eliminate. Measures of tubular secretory clearance predict kidney drug elimination, and lower estimated tubular secretory clearance is linked to the progression of CKD, cognitive decline, and mortality. Unfortunately, this complementary kidney function is, in many cases, unmeasurable with our current tools.
Key Research Question. How can tubular secretory clearance measurements enhance kidney function assessment, early detection of tubular disorders, and optimization of drug dosing?
Assess Kidney Function: Renal Stress Tests
Different types of physiologic stress tests can provide valuable insights into kidney function.
The furosemide stress test assesses renal tubular integrity and predicts progression in patients with stage 1 and 2 AKI. Furosemide administration has been evaluated for its effects on kidney oxygen consumption as a method to study CKD fibrosis and progression, which has differentiated ischemic kidneys from those with tubular injury.
Evaluating tubular function through dynamic physiological stress tests is essential for a comprehensive understanding of kidney function. Methods such as measuring proximal tubular secretion, assessing acid-base handling, and other physiological measures (e.g., water restriction/loading to assess concentrating and diluting ability, sodium MRI for sodium handling, and “tubular maximum” testing to determine reabsorptive limits for specific solutes. These approaches are particularly relevant in CKD, where the proximal and distal tubules may be affected differently, with important implications for both prognosis and treatment.
Declines in GFR commonly occur when renin-angiotensin system inhibitors (RASi) are initiated. A decline in eGFR of ≤13% over 3 months or ≤21% over 1 month has been associated with a lower risk of kidney failure. In patients with cardiac dysfunction, a decrease in eGFR of ≥20% at 14 days was not associated with adverse prognostic significance. Moreover, in patients who continued RAS inhibition, a survival advantage was maintained. Notably, those patients who displayed preserved glomerular hemodynamic function experience the best clinical outcomes. In contrast, one study found a relationship between adverse cardiorenal outcomes and creatinine rises of less than 30%.
Key Research Question. How can the kidney's responses to stressors, such as RAAS inhibition and dietary acid loads, be used to evaluate kidney health, identify functional limitations and affected compartments, determine disease subtypes, predict disease progression, and guide treatment?
Measuring KFR
The capacity of the kidneys to increase glomerular filtration rate (GFR) in response to increased demands or stress is termed kidney filtration reserve (KFR). This response can be physiological (as in pregnancy or unilateral nephrectomy) or persistent (as in obesity and diabetes), the latter of which is often maladaptive and has been implicated in the progression of kidney damage. This measurement provides insight not only into subclinical nephron loss but also into the interpretation of elevated GFR, particularly in hyperfiltration states.
In individuals with an elevated baseline GFR, a blunted or absent KFR following a standardized stress test suggests that the kidneys are already functioning near their maximal capacity, indicating a loss of reserve. One common method to measure KFR involves administering a protein load and observing the subsequent increase in GFR. A low KFR value (<15 ml/min per 1.73 m²) has been associated with an increased likelihood of developing acute kidney injury (AKI) or progressive chronic kidney disease (CKD).
KFR could be a promising tool for the early detection of subclinical kidney disease, facilitating preemptive therapeutic interventions, and its assessment could be valuable for monitoring kidney recovery following AKI. We need to develop a standard protocol for testing, including the interpretation of results, to drive the adoption of therapeutics that slow eGFR decline.
Key Research Question. How can kidney functional reserve (KFR) be quantified and applied to predict and prevent adverse kidney outcomes like AKI and CKD progression?
Glomerular function, albuminuria, and kidney disease progression
The glomerulus allows extensive fluid filtration while restricting the passage of macromolecules. The glomerular filtration barrier consists of 3 layers, one of which is the podocytes that closely envelope the glomerular capillaries through foot processes that interdigitate with those of adjacent podocytes. The luminal pressure in the capillaries required for fluid filtration exerts physical forces on the capillary wall that are counteracted by the GBM and podocytes. In a gel compression model of glomerular ultrafiltration, podocytes take on a more simplified architecture when injured and slit-diaphragm length is reduced, resulting in a smaller filtration slit area and a decline in the GFR of water and small solutes. The altered forces generated by the compression model cause podocytes to detach if the mechanical stress exceeds the threshold.
The mechanisms whereby the normal glomerular capillary wall restricts the passage of proteins while offering little resistance to the filtration of water and small solutes is named permselectivity. Quantification of permselectivity is important because it is associated with progression to kidney failure. Two methods evaluate permselectivity; the first is the dextran sieving curves, which characterize a change in glomerular permselectivity. These curves may be modeled through a small number of parameters, which include the shunt magnitude ω0, which is the fraction of the total glomerular filtrate that passes through parts of the filtration barrier with essentially no restriction to the passage of large molecules. The hazard ratio was 1.55 for each SD increment in ω0. Disadvantages: invasive, time-consuming, and not currently feasible for routine clinical use.
The other method is the selectivity index, which predicts the responsiveness of the individual patient to steroid therapy. The NIDDK workshop suggested that this selectivity index might be a reasonable surrogate (inverse) predictor of ω0, and also that a physical interpretation of the permselective shunt may reflect an early transient detachment of podocyte foot processes from the filtration surface. Standardization, broader use, and further study of the selectivity index (as a predictor of ω0) have the potential to identify early pathogenesis and clinically meaningful subtypes of proteinuria, as well as refine the assessment of treatment response.
Key Research Question. How can the glomerular selectivity index and perm selective shunt parameter (ω0) predict kidney disease progression, assess treatment efficacy, and evaluate podocyte health?
Novel Complementary images/biomarkers for Kidney Function Assessment
Functional imaging studies have complemented our understanding of physiological and pathological processes. However, the majority of techniques are limited by variability in platforms, protocols, and image analysis. Table 2.
Blood oxygen level–dependent MRI, Diffusion-weighted imaging MRI, Magnetic resonance relaxometry, and the Arterial spin labeling MRI are part of new tools. The Arterial spin labeling, for example, quantifies renal blood flow without contrast agents, capturing a fundamental aspect of kidney function as perfusion supports filtration and tubular processes.

Table 2: Functional imaging modalities in Kidney assessment
Key Research Question. How can advanced functional imaging modalities be combined with clinical data to reliably assess kidney function, improve early detection, risk stratification, therapy monitoring, and guide clinical decisions while addressing challenges
Currently, there are established and investigational urinary biomarkers that complement kidney function assessment, offering the advantage of providing a non-invasive and sensitive measure of kidney function. Table 3a and 3b. However, challenges remain regarding their validation and standardization. The integration of multi-marker panels is promising for advancing precision nephrology and enabling personalized patient care, particularly in addressing issues related to accessibility and variability.


Table 3: Established and emerging urine biomarkers
Conclusion
The reimagining kidney function assessment workshop, by the NIDDK, addresses the shortcomings of current methods. Kidney function assessment has long relied on two familiar pillars: eGFR and proteinuria, which provide an incomplete picture of kidney health, missing early signs of dysfunction and masking the kidney's intrinsic compensatory abilities; notwithstanding, these markers remain indispensable. This limitation has sparked tools that aim at enabling earlier detection, personalized interventions, and optimized outcomes. The NIDDK emphasized the urgent need to move beyond these traditional metrics and adopt a more comprehensive approach that includes multiple aspects of kidney function. So, how can we better measure, understand, and act upon the true complexity of kidney function? How can the use of various kidney function measures, tailored to the clinical scenario, help identify affected kidney compartments, disease subtypes, and treatment responses, as needed to implement precision medicine practices? The future of determining renal dysfunction will move well beyond looking at the kidney as just a one-dimensional filter.



Comments